One of the most important breakthroughs in modern migraine care has been the development of CGRP monoclonal antibodies (mAbs). These medications are the first treatments created specifically to prevent migraine, rather than being adapted from drugs used for other conditions.
For people who have struggled with older preventives due to side effects or limited benefit, CGRP monoclonal antibodies offer a highly effective, well-tolerated, and targeted option. For many patients, they represent a turning point in migraine control.
What Is CGRP and Why Does It Matter in Migraine?
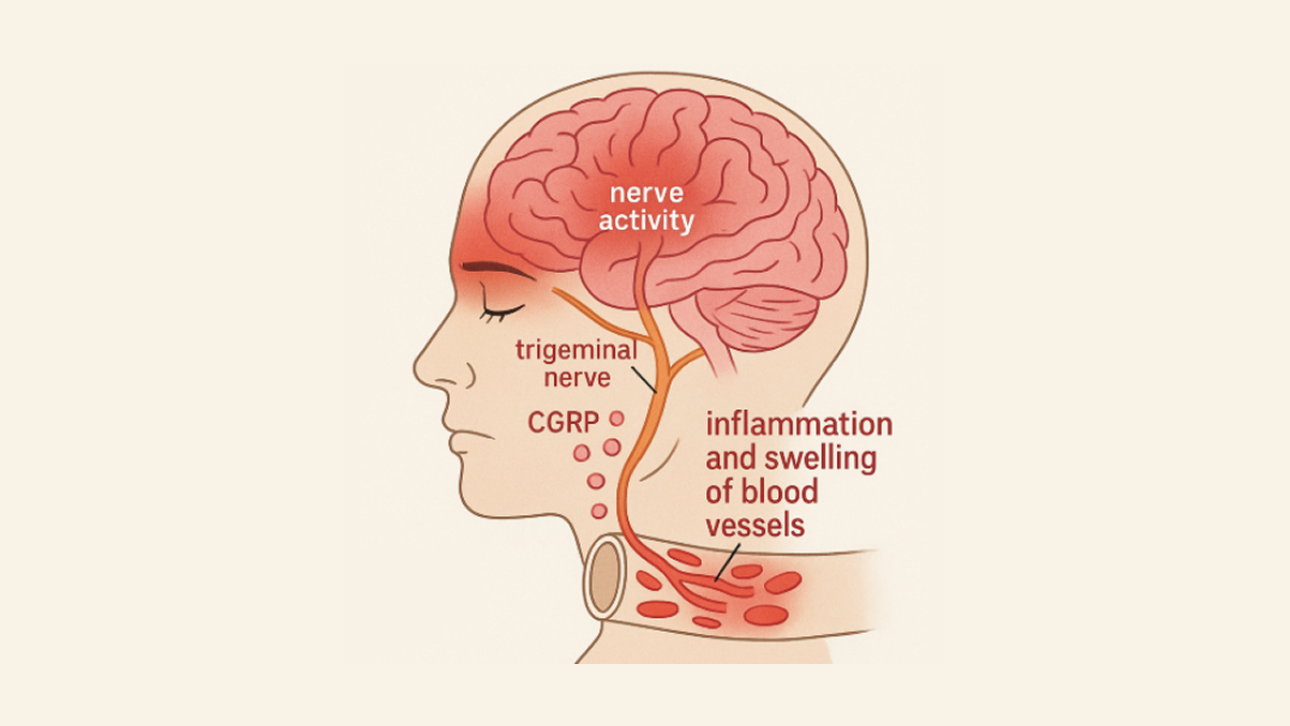
CGRP stands for calcitonin gene-related peptide, a neuropeptide that plays a central role in migraine biology. During a migraine attack, CGRP is released from nerve endings in the brain and surrounding tissues.
CGRP contributes to migraine by:
- Dilating blood vessels in the brain
- Increasing inflammation around pain-sensitive nerves
- Amplifying and sustaining pain signals
By blocking CGRP or its receptor, these medications interrupt the migraine process at a very early stage. This reduces the brain’s sensitivity to triggers and lowers the likelihood that a migraine attack will start.
The Available CGRP Monoclonal Antibodies
There are currently four CGRP monoclonal antibodies approved for migraine prevention.
- Aimovig (erenumab): Blocks the CGRP receptor
- Ajovy (fremanezumab): Binds directly to the CGRP molecule
- Emgality (galcanezumab): Binds directly to the CGRP molecule
- Vyepti (eptinezumab): Binds CGRP and is given intravenously every three months
All four are highly specific. They act almost exclusively on the migraine pathway, which explains their favorable side-effect profile compared with many older preventive medications.
Evidence for Effectiveness
Clinical trials and real-world studies consistently show strong benefits from CGRP monoclonal antibodies.
Key findings include:
- An average reduction of 4–8 monthly migraine days
- About 50% of patients achieve at least a 50% reduction in migraine frequency
- A subset of patients experience near-complete remission
- Benefits often begin within the first month, with continued improvement over time
Importantly, these results are seen in both episodic and chronic migraine, including patients who have failed multiple traditional preventive therapies.
How CGRP Monoclonal Antibodies Are Given
The method and frequency of dosing varies slightly between medications.
- Aimovig, Ajovy, and Emgality are given as subcutaneous injections
- Usually once monthly
- Ajovy also offers a quarterly dosing option
- Vyepti is given as an intravenous infusion every three months, administered in a clinic
Most patients who use injections are able to self-administer at home after brief training, using prefilled pens or syringes.
Side Effects and Safety
CGRP monoclonal antibodies are generally very well tolerated. The most commonly reported side effects include:
- Injection site reactions such as redness, swelling, or itching
- Constipation, particularly with erenumab (Aimovig)
- Rare allergic reactions
Unlike many older migraine preventives, CGRP mAbs:
- Do not cause sedation
- Do not cause weight gain
- Do not cause cognitive or memory problems
They are also considered safe for most patients with cardiovascular disease, as they do not constrict blood vessels. Long-term safety data is reassuring, with many patients using these treatments for years without significant issues.
Who Should Consider CGRP Monoclonal Antibodies?
CGRP monoclonal antibodies may be especially helpful for:
- People with frequent or chronic migraine
- Patients who have tried and failed two or more traditional preventive medications
- Those who cannot tolerate side effects from oral preventives
- Patients who prefer once-monthly or quarterly dosing over daily pills
Many insurance plans require documentation of prior preventive failures before approving coverage.
Access and Coverage in Canada
Cost remains one of the main barriers to CGRP monoclonal antibodies. These medications can cost hundreds of dollars per month without coverage.
In Canada:
- Most private insurance plans cover CGRP mAbs with prior authorization
- Some provincial programs provide coverage for patients who meet strict criteria, such as chronic migraine and multiple preventive failures
- Manufacturer patient support programs often assist with coverage navigation, training, and co-pay support
Working closely with a healthcare provider helps streamline the approval process.
Practical Tips for Patients Using CGRP Monoclonal Antibodies
- Expect gradual improvement: Some benefit may appear quickly, but give treatment 3–6 months before judging success
- Track headache days: Headache diaries help document response and support insurance renewals
- Store properly: Most injections require refrigeration, with limited room-temperature allowance before use
- Rotate injection sites to reduce irritation
- Maintain follow-up appointments to reassess dosing, effectiveness, and access
Lifestyle measures such as regular sleep, hydration, and stress management continue to support medication effectiveness.
Take-Home Message
CGRP monoclonal antibodies represent a major advance in migraine prevention. By directly targeting the biology of migraine, they provide effective, well-tolerated, and convenient options for people who have struggled with traditional therapies.
Although cost and access can be challenges, for eligible patients these treatments can be life-changing—reducing migraine frequency, improving daily function, and restoring a sense of control over life with migraine.