
For decades, migraine was viewed as a problem of blood vessel dilation and constriction — a purely vascular issue. But science now paints a far more complex picture. Migraine is a neurological disorder that involves multiple brain networks controlling pain, sensory input, and blood vessel function.
Understanding what happens in the brain during a migraine attack helps explain why the symptoms go far beyond head pain — and why effective treatment requires more than just pain relief.
The Brain’s Sensory Overload
The migraine brain is hypersensitive to stimulation. Light, sound, smell, or even mild touch can feel unbearable during an attack. This sensory overload comes from neuronal hyperexcitability — nerve cells that fire more easily and spread signals more widely than in non-migraine brains.
This explains why migraine feels like a sensory storm, not “just a headache.” Everyday experiences become overwhelming because the brain’s sensory filters are malfunctioning. Research published in Neurology Journal shows that this hyperexcitability can persist even between attacks, helping explain lingering sensitivity for some people.
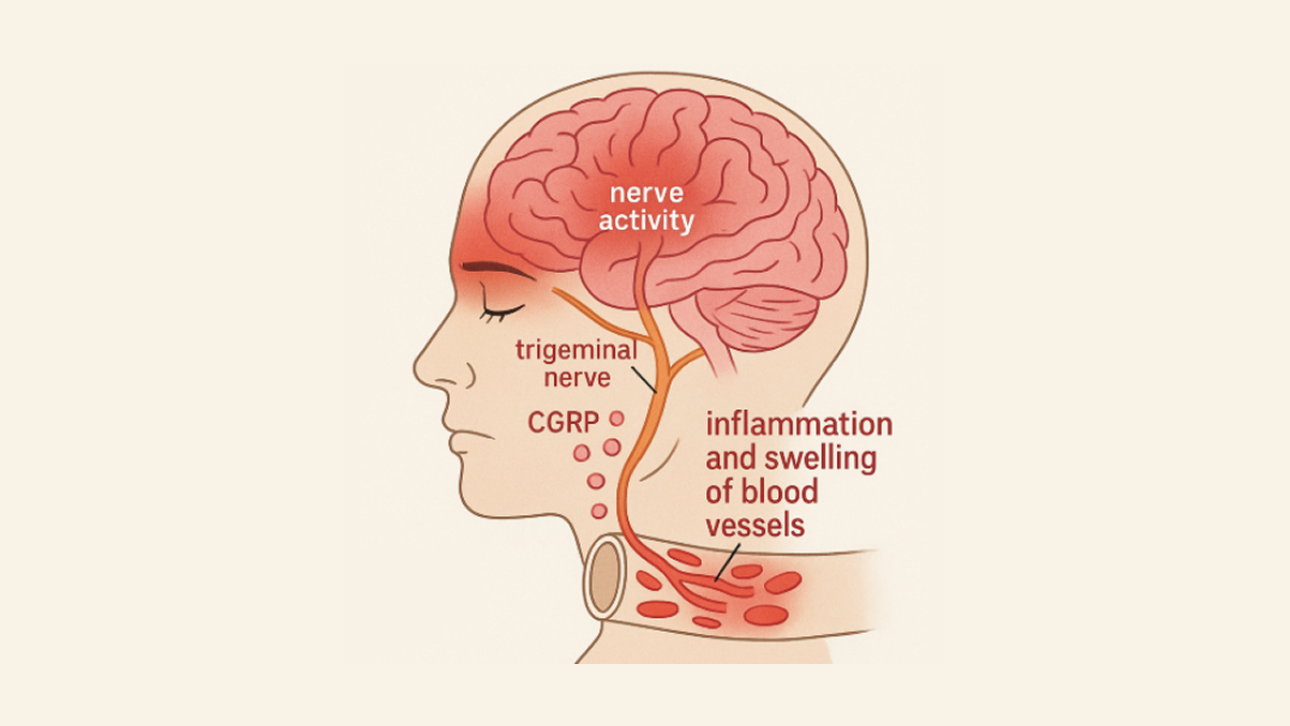
The Role of the Trigeminovascular System
At the center of migraine biology lies the trigeminovascular system, a network of pain-sensitive nerves surrounding the brain’s blood vessels and protective coverings (the meninges).
When activated during a migraine, these nerves release pain-signaling chemicals such as calcitonin gene-related peptide (CGRP), substance P, and neurokinin A. These neuropeptides trigger blood vessel dilation and cause sterile neurogenic inflammation — a type of swelling that heightens pain signals without infection.
This process amplifies pain messages traveling to the brain, creating the throbbing, pulsating headache migraine is famous for.
Did you know? CGRP-targeting medications were developed specifically to block this pain pathway — a breakthrough that stemmed directly from this biological discovery.
Cortical Spreading Depression and Aura
For those who experience migraine aura, a phenomenon called cortical spreading depression (CSD) plays a key role.
CSD is a slow wave of electrical activity that moves across the brain’s surface, followed by a temporary reduction in activity. The symptoms depend on where this wave travels:
- Across the visual cortex → flashing lights or zigzag patterns
- Through the sensory cortex → tingling or numbness
- Over language areas → temporary speech problems
Though harmless, this electrical storm explains the evolving neurological symptoms that can precede or accompany a migraine attack.
Brainstem Involvement: The Migraine Control Center
Modern brain imaging reveals that the brainstem — particularly areas like the dorsal pons and periaqueductal gray — shows abnormal activity during migraine attacks.
These regions regulate pain and sensory processing, acting as “control hubs” for how the brain responds to incoming stimuli. When these centers misfire, symptoms such as neck stiffness, fatigue, nausea, and light sensitivity may appear — even before the headache starts.
Why Migraine Symptoms Extend Beyond Pain
Because migraine is a whole-brain disorder, symptoms affect multiple systems:
- Nausea and vomiting: Triggered by activation of brainstem centers that control the gut.
- Light and sound sensitivity: Caused by overactive visual and auditory pathways.
- Cognitive fog: Linked to disrupted attention and memory circuits.
- Fatigue and mood changes: Reflect altered energy and emotional regulation networks.
These wide-ranging effects highlight that migraine is not just pain in the head — it’s a complex neurological event involving many parts of the brain.
The Role of Genetics in Migraine Susceptibility
Migraine often runs in families. Around 70% of people with migraine have a close relative with the condition.
Research published in Cephalalgia and The Lancet Neurology has identified numerous genetic variants linked to migraine, many involving ion channels — proteins that help nerve cells communicate. These inherited differences create a “migraine-prone brain”, more easily tipped into attack mode by stress, hormones, dehydration, or lack of sleep.
How Biology Shapes Modern Migraine Treatment
A deeper understanding of migraine biology has revolutionized treatment options. Therapies now target specific pathways in the brain and nerves rather than simply masking pain:
- CGRP-targeting therapies: Such as Aimovig, Ajovy, Emgality, and Vyepti, which block CGRP’s pain-signaling effects.
- Triptans: Serotonin receptor agonists that reduce trigeminal nerve activation and inflammation.
- Botox: Reduces neurotransmitter release in overactive pain circuits.
- Neuromodulation devices: Use gentle electrical or magnetic stimulation to calm hyperactive brain regions.
These therapies underscore how far migraine treatment has evolved — from treating blood vessels to directly targeting brain networks.
Practical Steps for Patients
Understanding migraine biology empowers patients to take more informed steps in managing their condition:
- Track symptoms carefully: Record sensory, cognitive, and emotional symptoms — not just pain intensity.
- Recognize triggers in context: Triggers like stress or sleep loss don’t cause migraine, but they can tip an already sensitive brain into attack.
- Pay attention to aura and prodrome: These are neurological warning signs, not psychological weaknesses.
- Stay informed about new therapies: Many of the latest treatments are based on cutting-edge neuroscience.
Take-Home Message
Migraine is a disorder of brain networks, not just blood vessels. Abnormal nerve signaling, cortical spreading depression, brainstem dysfunction, and neuropeptide release all contribute to the experience of an attack.
By understanding the biology of migraine, both patients and clinicians can better appreciate why symptoms vary so widely — and why personalized, brain-focused treatments offer real hope for long-term relief.
Explore More on Our Site
If you found this guide helpful, explore these related posts to deepen your understanding of migraine and other headache disorders: