For many people living with migraine, the pain is only one piece of a much larger puzzle. Nausea and vomiting—symptoms reported by up to 90% of people during attacks—can be just as disabling as the headache itself. These symptoms make it harder to take oral medications, worsen dehydration, and dramatically affect day-to-day function. Fortunately, anti-nausea medications in acute migraine care offer real relief and can even help your other treatments work better.
Why Nausea Matters in Migraine
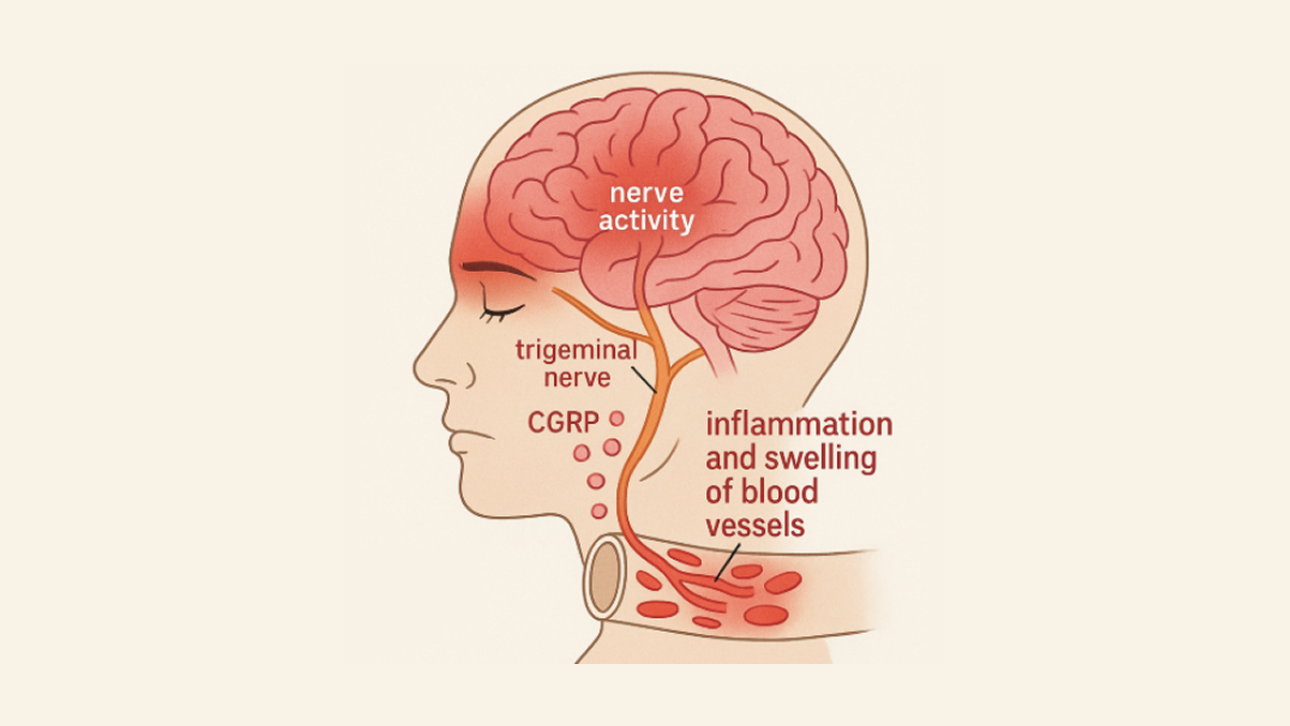
Nausea is far more than an annoying side effect. During a migraine attack, the brainstem can disrupt how the stomach functions, slowing digestion and creating hypersensitivity in the gut. This process—called migraine-related gastroparesis—directly affects how well medications are absorbed and how quickly symptoms escalate.
Many patients experience vomiting during attacks, which makes it almost impossible to keep oral medications down.
Even when vomiting doesn’t occur, delayed stomach emptying can severely reduce how effectively migraine medications work.
Persistent nausea adds its own layer of suffering, increasing disability and making attacks feel longer and more intense.
Because of these factors, tackling nausea head-on often improves comfort and boosts the effectiveness of other migraine treatments.
Commonly Used Anti-Nausea Medications for Migraine
Several antiemetics are used alongside migraine-specific treatments like triptans. Each option works differently, and the best choice often depends on your symptoms and medical history.
Metoclopramide (Maxeran, Reglan)
Metoclopramide is one of the most widely used anti-nausea medications for migraine. It works by blocking dopamine receptors in the brain and speeding up stomach emptying—both helpful during attacks.
It can be taken orally, intravenously, or intramuscularly, which makes it especially useful when nausea affects medication absorption.
In many emergency departments, intravenous metoclopramide is part of the standard migraine treatment toolkit thanks to its dual benefit for both pain and nausea.
Prochlorperazine (Stemetil, Compazine)
Prochlorperazine is another dopamine-blocking medication with strong anti-nausea and anti-migraine properties.
It is commonly administered intravenously or intramuscularly in hospitals and emergency settings, though oral and suppository forms can also be prescribed for home use.
For some patients who cannot take triptans or find them ineffective, prochlorperazine may serve as a standalone acute treatment.
Domperidone (Motilium)
Domperidone improves stomach motility and reduces nausea, with the added benefit of causing fewer central nervous system side effects because it does not cross the blood–brain barrier easily.
It is available orally in Canada and is often used when nausea interferes with reliable absorption of other oral medications.
Ondansetron (Zofran)
Ondansetron is a 5-HT3 serotonin receptor antagonist widely used to treat chemotherapy-induced nausea.
While it works well for migraine-related nausea, current evidence suggests it may be less effective for overall migraine pain relief compared to dopamine-blocking antiemetics.
It is a helpful option for people who cannot tolerate medications like metoclopramide or prochlorperazine.
Effectiveness of Anti-Nausea Medications in Migraine Treatment
Anti-nausea medications do more than settle the stomach—they can directly improve migraine outcomes.
Research shows that both metoclopramide and prochlorperazine can relieve migraine pain in addition to nausea, making them powerful dual-purpose treatments.
In emergency departments, intravenous prochlorperazine has been shown to outperform opioids for migraine relief, offering faster and more reliable results without the risk of opioid-related side effects.
Because antiemetics can improve stomach emptying, they also enhance the absorption of migraine medications like triptans—especially when taken early in an attack.
Side Effects and Safety Considerations
While anti-nausea medications are widely used and generally well tolerated, they do come with potential side effects.
Metoclopramide and prochlorperazine may cause drowsiness, dizziness, or restlessness. In rare cases, they can trigger movement-related side effects—such as dystonia or akathisia. These effects are typically short-lived and can be prevented or treated with supportive medications.
Domperidone carries a small risk of heart rhythm changes (QT prolongation). Because of this, clinicians avoid prescribing it to people with known cardiac conditions unless the benefits clearly outweigh the risks.
Ondansetron is usually well tolerated, but constipation, headache, or mild dizziness can occur.
Your clinician will help determine the best choice for you based on your history, current medications, cardiovascular status, and how your migraine attacks typically unfold.
How Anti-Nausea Medications Are Used in Migraine Care
Anti-nausea medications can be used in several ways depending on the severity and timing of symptoms.
At Home
Many people are prescribed oral domperidone or metoclopramide to take alongside a triptan or NSAID—especially if nausea reliably accompanies their attacks.
Hospital or Emergency Care
For moderate to severe attacks, intravenous metoclopramide or prochlorperazine are commonly used. They may be combined with IV fluids and sometimes diphenhydramine to reduce the risk of restlessness or akathisia.
Rescue Therapy
For people whose oral medications fail due to vomiting, antiemetics can be an essential component of a “rescue plan,” ensuring relief even when oral treatments are not an option.
Who Benefits Most from Anti-Nausea Medications?
Anti-nausea medications can be especially helpful for:
- People whose attacks routinely involve nausea or vomiting.
- Individuals who experience unreliable absorption of oral triptans due to delayed stomach emptying.
- Patients needing emergency treatment for severe or unrelenting attacks.
- Anyone seeking non-opioid alternatives in hospital settings.
Practical Tips for Patients
Open communication with your healthcare provider can help you get the most out of anti-nausea therapy.
Talk about nausea early. Many people focus solely on pain when describing symptoms, but nausea is a critical factor in choosing the right treatment strategy.
Combine treatments when needed. Using an antiemetic alongside an acute migraine medication can make both more effective.
Explore alternate formulations. If swallowing pills during an attack is difficult, consider dissolvable tablets, suppositories, or injectable forms.
Watch for side effects. Report restlessness, unusual movements, or heart palpitations—these issues are usually manageable with quick adjustments to therapy.
Plan in advance. If nausea reliably accompanies hormonal or menstrual migraines, having your antiemetic ready can prevent escalation.
Take-Home Message
Nausea is one of the most disabling aspects of migraine, but it is also one of the most treatable. Anti-nausea medications such as metoclopramide, prochlorperazine, domperidone, and ondansetron can improve comfort and significantly enhance the effectiveness of migraine-specific treatments.
By addressing nausea proactively, many people experience shorter attacks, better response to medication, and fewer emergency visits—leading to meaningful improvements in quality of life.